692
Views & Citations10
Likes & Shares
INTRODUCTION
We believed studying animals susceptible to colonization with H. pylori would greatly facilitate the
studies aimed at clarifying its pathogenicity. Such a test model is
advantageous in that the animals are easy to handle, widely available, and
inexpensive, thus permitting a wide variety of experiments to be carried out.
As a result, we achieved continuous colonization with H. pylori in the gastric mucosa of nude mice and euthymic mice in
1990 [2], using freshly isolated strains of H.
pylori obtained from patients with gastritis, gastric ulcer, and duodenal
ulcer. Moreover, we developed the H.
pylori infected rodent model using a Mongolian gerbil which was observed
severer inflammation and the ulceration in 1996 [3]. In addition, the gastric
mucosa would not be colonized unless freshly isolated strains of H. pylori was used, by the established
strains.
To establish the H. pylori
infected mouse model, the challenged H.
pylori inocula such as two-milliliter aliquots of the culture fluid of H. pylori with a concentration of 108
organisms/ml (adjusted as the report) were prepared on a one-time basis.
This H. pylori infected model
to which extraordinary high concentrated inocula is administered is one of the H. pylori infected case by the oral
transmission of H. pylori which is
unrealistic large amount of H. pylori.
Then, what is the source of natural H.
pylori transmission in case of oral transmission? One example is H. pylori infected human. However, this
source is not highly concentrated H.
pylori. Therefore, it is speculated that the intimate interaction is
required for H. pylori transmission.
There have been several reports about the mode of transmission of H. pylori. It is suggested that the
representative route of H. pylori
transmission is presumably close personal contact, as mentioned above, special
among the familial members. Instead of demonstrating the H. pylori transmission among the humans, we demonstrated the H. pylori transmission from challenged
to non-challenged mice in a single cage using the mouse model we developed
previously [2].
The results [4] are following:
Six mice were challenged with H.
pylori inocula; one group consisted of one challenged mouse 1 week after
inoculation raised with four non-challenged mice in a single cage. For the
single cage, a polycarbonate cage or a mesh floor cage was used. The three
groups were kept in a polycarbonate cage and the other three groups kept in a
mesh floor cage to avoid H .pylori transmission
through stool. During 3 weeks after co-raising of H. pylori challenged and non-challenged mice, H. pylori was detected in the stomachs in 3 of 12 non-challenged
mice in the polycarbonate cage and in 2 of 12 non-challenged mice in the cage
with a steel mesh floor. H. pylori
was detected from saliva or stool in two non-challenged, infected mice in the
polycarbonate. Moreover, RAPD fingerprinting of the total five strains isolated
from five non-challenged infected mice both cages showed the same pattern and
concordance with that of the challenged strain and the strains isolated from
challenged mice. After coraising for 1 or 2 weeks, H. pylori was detected in the stomach in only 1 of 48
non-challenged mice in both cages.
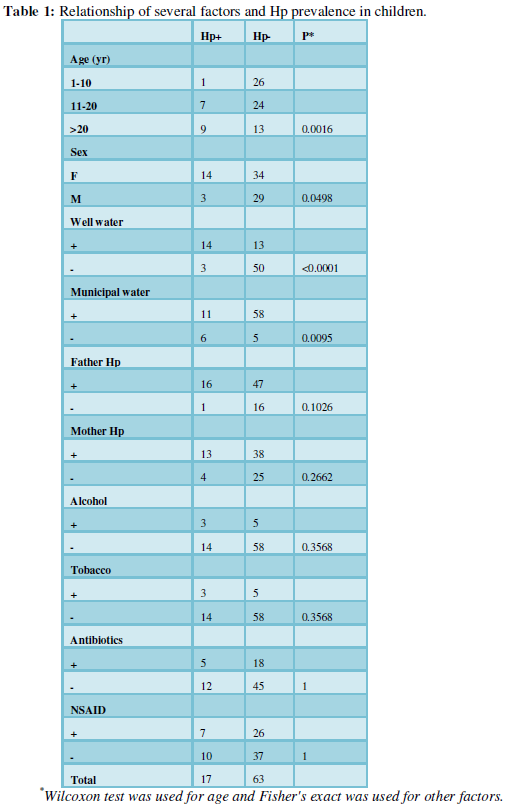
The Hp (H. pylori) status of
their 82 parents (41 fathers and 41 mothers) was positive in 57 (32 males and
25 females) and negative in 25 (9 males and 16 females). The Hp status of the
parents had the same trend according to the age. The relationship between
several factors and Hp infection of children (17 positive and 63 negative) was
evaluated as shown in Table 1.
In spite of Japan being a developed country, the reported prevalence of
H. pylori infection is higher than
that of other developed countries. This indicates that many houses have private
wells and had drunk well water rather than the municipal water with good
sanitation 35 years ago in Japan. Municipal water with good sanitation was
available to 69.4% of Japan at that time. The availability of municipal water
was increased about 5% every 5 years and reached 94.7% in 1990 and increasing
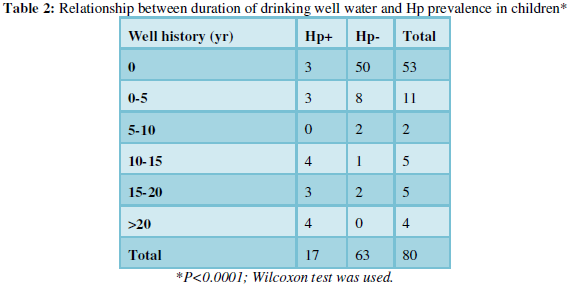
in subsequent years. It is speculated that most H. pylori transmission in Japan depends on waterborne transmission
and the occurrence of its transmission is strongly associated with the duration
of the history of drinking well water.
CONCLUSION
1. Warren JR, Marshall B (1983) Unidentified
curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1:
1273-1275.
2. Karita M, Kouchiyama T, Okita K, Nakazawa T
(1991) New small animal model for human gastric Helicobacter pylori infection: Success in both nude and euthymic
mice. Am J Gastroenterol 86: 1596-1603.
3. Matsumoto S, Washizuka Y, Matsumoto Y, Tawara
S, Ikeda F, et al. (1997) Induction of ulceration and severe gastritis in Mongolian
gerbil by Helicobacter pylori infection.
J Med Microbiol 46: 391-397.
4. Karita M, Matsumoto S, Kamei T, Shinohara K,
Sugiyama T (2005) Direct transmission of H.
pylori from challenged to non-challenged mice in a single cage. Digest Dis
Sci 50: 1092-1096.
5. Hulten K, Enroth H, Engstrand L (1998)
Presence of Helicobacter species DNA
in Swedish water. J Appl Microbiol 85: 282-286.
6. Karita M, Teramukai S, Matsumoto S (2003)
Risk of Helicobacter pylori transmission
from drinking well water is higher than that infected intrafamilial members in
Japan. 48: 1062-1067.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)


